Power driven instruments
Basic principles of use
Modern power-driven instruments are as effective as hand instruments in removing of biofilm, extrinsic stains and calculus deposits. An instrument tip, vibrating at a high-frequency, provides mechanical force for effective cleaning. Power driven instruments such as ultrasonic and sonic, are comprised of a handpiece and a tip, or an insert. Ultrasonic/sonic tips/inserts with large-sized working ends are limited to supragingival use. Finer tips/inserts provide access to deep periodontal pockets and are used for subgingival debridement. The working end of a thin power-driven instrument is significantly smaller in size than the working-end of a hand-activated standard curette. Thin ultrasonic/sonic tips are similar in size to calibrated periodontal probes and provide excellent accessibility for debridement of periodontal pockets and furcations.
A constant stream of fluid that runs through the handpiece provides a flushing action that removes debris from the treatment site. ‘Acoustic turbulence’ and ‘cavitation’ are additional effects produced by the power-driven instruments that have antimicrobial effect.
Less pressure and less time as well as less detrimental effect on soft and hard tooth structures are other advantages of power-driven over hand instruments.
There are two types of power-driven instruments: sonic and ultrasonic.
Sonic handpieces attach to the dental unit’s compressed air line and operate at 3 000 to 8 000 cycle per second (cps), 3-8 kHz.
Ultrasonic instruments have an electric generator and operate at 18 000 to 50 000 cps (18 to 50kHz).
There are two types of ultrasonic instruments: magnetostrictive that produce elliptical or circular
motions of the tip and piezoelectric that produce linear ones.

Contraindications for use
(Niled_Gehrig JS. 2008)
1. Communicable disease that can be disseminated by aerosols (e.g. flu, hepatitis, tuberculosis, respiratory infections)
2. High susceptibility to opportunistic infections that can be transmitted by contaminated aerosols (e.g. immunosuppressed patients, debilitated patients with chronic medical conditions, uncontrolled diabetes)
3. Respiratory or pulmonary disease or the patients who experience difficulties in breathing (e.g. severe asthma, cystic fibrosis, severe emphysema)
4. Certain styles of cardiac pacemakers may be affected by magneto strictive ultrasonic. Newer pacemakers have built in shields that make ultrasonic instrumentation safe.
Piezoelectric ultrasonic devices do not interfere with pacemaker functioning.
5. Compromised or lessened gag reflex or difficulties in swallowing (e.g. multiple sclerosis, muscular dystrophy or paralysis)
6. Dental conditions (i.e. porcelain crowns, composite resin restorations, demineralized enamel surfaces, dentinal hypersensitivity)
7. Implants, unless the ultrasonic tip is covered with a specially designed plastic sleeve
8. Primary or newly erupted teeth
(Niled_Gehrig JS. 2008)
Suggested reading
Arabaci T, Ciçek Y, Canakçi CF. Sonic and ultrasonic scalers in periodontal treatment: a review. Int J Dent Hyg. 2007;5(1):2–12. doi:10.1111/j.1601-5037.2007.00217.x
Supragingival scaling on anterior teeth
Supragingival scaling on posterior teeth
Supragingival scaling – clinical case
Subgingival scaling
(with power driven instrument – principles)
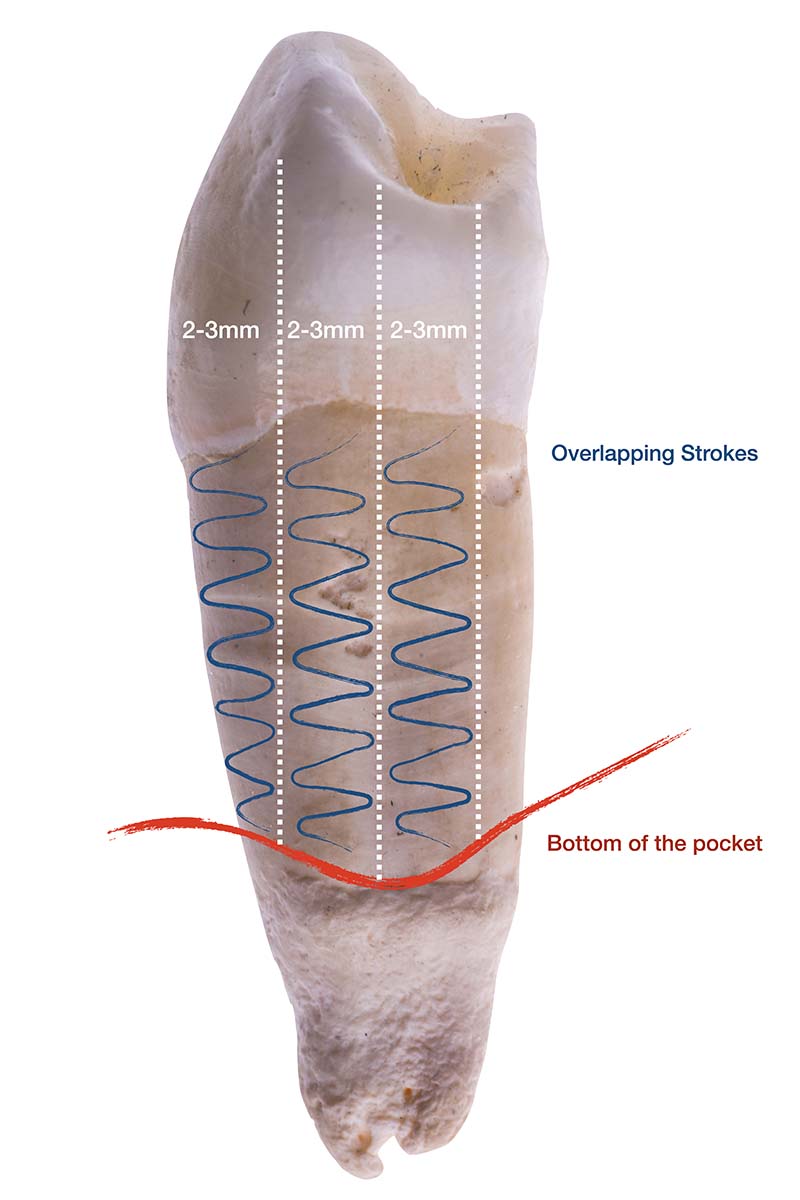
Steps:
1. The deepest part of the pocket of the respective site is detected using vertical strokes (with running instrument)
2. The removal of the calculus starts at the bottom of the pocket
3. The tip is then moved slowly towards the sulcus using horizontal/oblique strokes
4. Vertical detection strokes are used again to detect the neighbouring bottom of the pocket
5. The neighbouring 2-3mm is cleaned using horizontal/oblique strokes, slightly overlapping the former 2-3mm
Power driven instruments – Basic principles
Anterior teeth: FACING & AVERTED
Posterior teeth